The premature passing away of Annie made me ponder. It is said that only the good die young. They now dwell in paradise at the right hand of the Lord or have achieved moksha depending on ones beliefs. It is the ones who remain who suffer the loss. In this uncertain life there are but two constants, birth and death, in between these constants there are variables. I am in the sunset of my life and cannot be sure when the Grim Reaper knocks. My mother lived till the ripe age of 94 but when younger she wanted to see her children married, then to see her grandchildren, next her grandchildren married and finally her great grandchildren. She was blessed to live long enough to see it come to pass. It is said that our natural life sans diseases is determined by the length of telomeres at the end of the chromosomes. Telomeres are protective DNA caps at the ends of chromosomes. They act like the plastic tips on shoelaces, preventing chromosomes from fraying or sticking to each other. They shorten with each division till they become critically short and the cell stops dividing or dies. Two weeks ago I was in a Surgical Conference and attending a best paper presentation. My student had just finished presenting and during the next presentation a surgeon sitting two rows in front of me indicated to the judges on the stage that he was not feeling well. The judges rushed down and asked him to lie down on the sofa. He then had a cardiac arrest, immediate CPR was given and he was transferred to the hospital but he did not make it! He was the President of the Rajasthan Surgical Society and had come to canvass for his bid for President of the Association of Surgeons of India. Unfortunately that was not to be. I had met at lunch a day earlier and he looked hale and hearty. Not an inch of excess fat and a wiry build. Nagpur was shocked by the death of a young Neurosurgeon. He had a very successful career and had no ‘habits’ i.e. he did not smoke nor was he fond of Bacchus. He was seen in the gym 6 am without fail. His only failing if you can call it so was that he was a workaholic. I knew since the time he began his career and he built up an empire, recently he had purchased a plot for ₹23 crores but “man proposes and God disposes”. One of my colleagues who was just 3 years senior to me suddenly came down with severe myalgia, which progressed over a period of a month to myoglobinuria and renal failure followed by respiratory failure. He had to be put on an ECMO machine but he did not make it. Till the end nobody could figure out what exactly caused these sequence of events. He was again sans habits though overweight and not fond of movement, though no comorbidities. I have a young postgraduate student under me and a year ago she initially had a URI which rapidly progressed to respiratory failure and she had to be put on a ventilator. Luckily she lived to tell the tale but in her case too they could not pinpoint an organism, despite extensive testing. Because of her youth she came out of it. Then we all know about the sad passing away of Agroo in a freak accident. Absence of habits or a vegetarian diet does not necessarily endow one with immunity.Anecdotal In Hindi there is a saying, “जाको राखे सैया, मार सके ना कोई”, meaning Whom God protects, no one can kill or harm. We can count ourselves blessed to have made it thus far. “Cowards die a thousand deaths but the valiant taste of death but once”
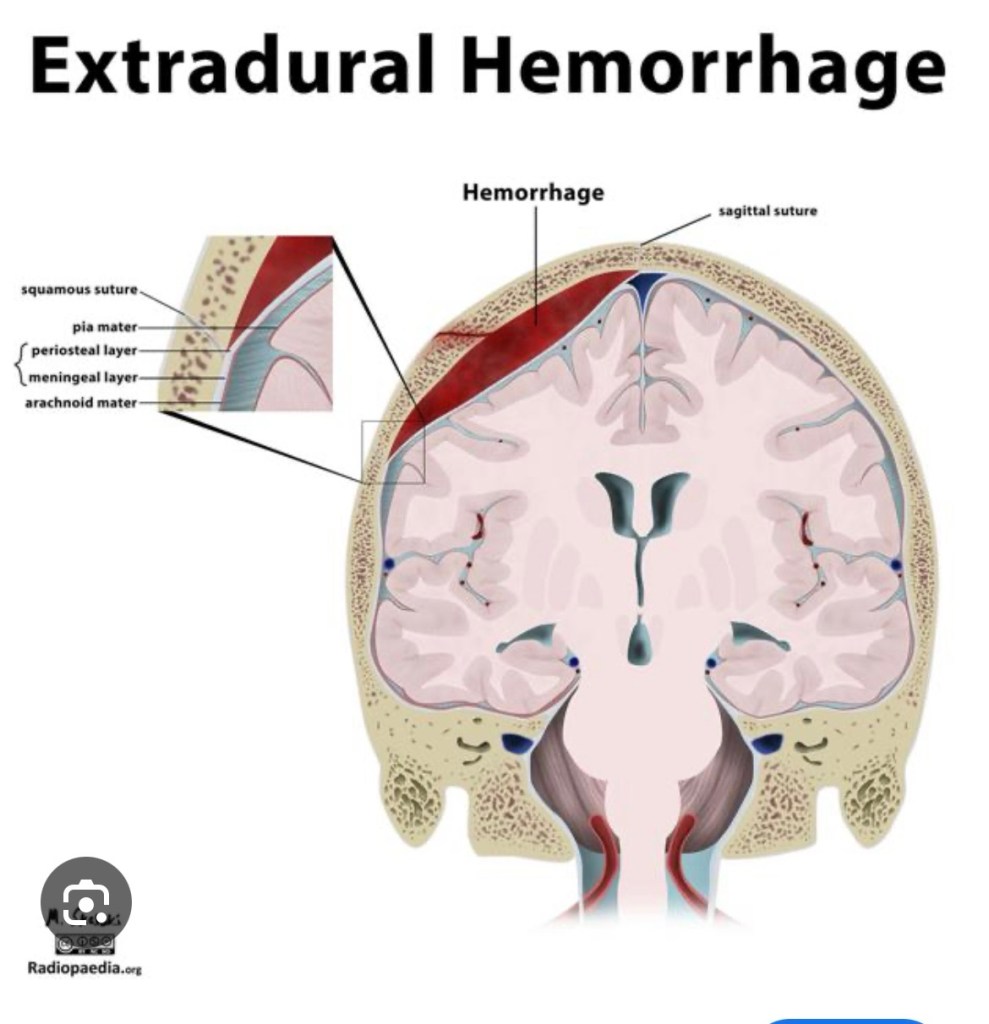
An extradural haematoma is a condition which happens after a head injury. It is a collection of blood that builds up in the space between the skull and the outer covering of the brain, the dura mater.
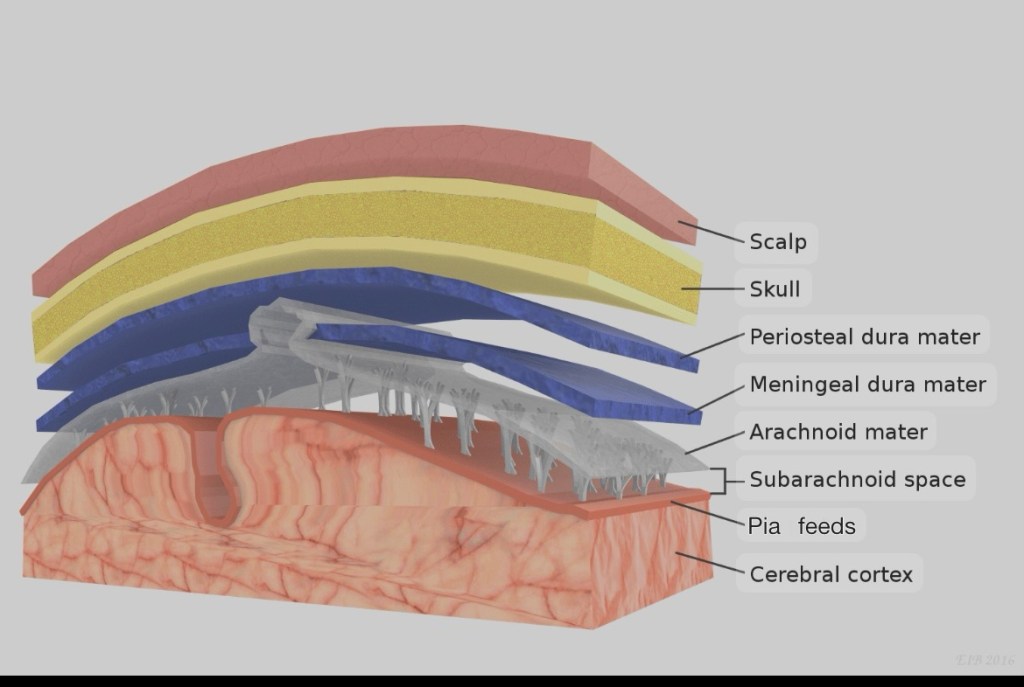
The brain is protected by several layers. First is the scalp, which is the tough skin covering the head. Under that is the skull, a hard bone that protects the brain. Beneath the skull are three layers called the meninges: the dura mater, arachnoid mater, and pia mater.
Layers covering the brain
The brain continues downward as the spinal cord, which passes through an opening at the base of the skull called the foramen magnum and into the spinal canal, which is made up of bones stacked on each other but interlinked called vertebrae. There are a total 33 vertebrae out of 5 are fused as the sacrum and 4 are fused as the coccyx. The stacked arrangement gives the spine flexibility, due the multiple joints. The meninges also cover the spinal cord.
The brain and the spinal cord float in a special fluid called cerebrospinal fluid (CSF), which helps cushion and protect them from injury.
After a head injury, a small fracture in the skull can sometimes tear a blood vessel on the surface of the dura mater—usually an artery called the middle meningeal artery. This causes bleeding in the space between the skull and the dura mater. The resultant expanding clot presses on the brain. The brain has the consistency of ‘Jello’ and can get easily compressed. At first, this pressure may compress the brain to the opposite side of the clot, and then downwards and out through the foramen magnum.
In essence the clot occupies the space previously occupied by the brain, by squeezing it out through the path of least resistance, the foramen magnum.
This wrecks havoc and initially causes headache, nausea and vomiting, followed by confusion and drowsiness progressing into a deepening coma.
There will be weakness of the body on the opposite side of the haematoma, because the right and left hemispheres of the brain control opposite sides of the body.
There will be a dilation of the pupil on the same side of the haematoma because as the brain is pushed to the opposite side, there’s traction on the 3rd cranial nerve as it emerges from the base of the brain and exits via another opening in the skull, the cavernous sinus to supply the eye. As the brain is pushed to the opposite side it gets stretched.
The good thing about extradural haematoma is that there is no injury to the substance of the brain, the symptoms are caused by the compression, hence timely evacuation of the haematoma would result in a complete recovery.
There is what is called the ‘lucid interval’ which occurs in 20%-50% of the cases. This is characterised by a period of lucidity between an initial brief period of loss of consciousness followed by a prolonged period of deepening coma.
Initially following the trauma to the head there’s a loss of consciousness due to ‘concussion’, which is a temporary loss of consciousness, following a head injury, with complete recovery and no neurological deficits.
The patient recovers from the concussion but due to the expanding clot in the extradural space, the patient again loses consciousness and progresses into a deepening coma.
‘Lucid interval’ though not present in all cases of extradural haematoma, if presents is highly indicative of an extra dural haematoma.
I did my surgical residency in Punjab, in the late 80s and 90s, when the secessionist movement was at it’s peak. Trauma a plenty with bombs exploding regularly in front of the police station near the hospital, terrorists opening gunfire in market places and on social gatherings. Once we treated a film crew who were shot at during the shooting of a Punjabi film, ‘Jatt te zameen’. The reigning superstar of the Punjabi film industry Veerendra Singh, who was starring was brought dead to the casualty. He was a cousin of Bollywood film star Dharmendra.
Then there were penetrating head injuries. Among the cases I can recollect there was a young man, who was shot in the head by a 12 bore gun. The cartridges of a 12 bore contain multiple pellets which didn’t penetrate the skull but were embedded all over the scalp. A 14 year old boy shot point blank with the muzzle of the 12 bore kept below his chin. One entire half of his face was blown away. His tongue hanging free and his epiglottis was visible opening and closing with each breath revealing the glottis.
The miraculous thing was both of them survived, the young boy underwent extensive surgery, lost one eye and ear and half of his face but lived to tell the tale.
Another case where a husband attacked his wife with an axe. He opened a good portion of the forehead exposing the frontal lobe of the brain. She too survived to put a case against her husband, for which I had to go to the court as a witness.
Then there were the blunt traumas to the head secondary to road traffic accidents and violence, the victims were invariably under the influence of alcohol and were extremely restless and sometimes violent. One was a boxer who had fallen off the back of a motorcycle, while riding pillion and sustained injury to the back of his head. He was disoriented and restless and almost impossible to restrain. He would easily lift off from the ground two orderlies trying to tie down each arm, like doing a pectoral fly but using two men instead of dumbbells in each hand.
In those days chlorpromazine, an anti psychotic drug was injected to calm down the patient.
Once sedated they could be taken for a Computed Tomography Scan (CT Scan) to assess for brain injuries. The reports could vary from brain contusions, subdural haematomas and of course extradural haematomas.
I was posted as surgery residents in Neurosurgery and as there was no post graduation program in the department of Neurosurgery, I had to fill that role. The pecking order was the Chief, the lecturer and then us. I got exposed to a variety of surgeries.
In neurosurgery like in any surgery the first step is the exposure of the area of interest. In abdominal surgeries the abdomen has to be opened in order to operate, similarly in neurosurgery the skull has to be opened or craniotomy over the required area for the surgical procedure to be performed.
Surgeries had to be performed with the patient in various positions depending on the location of the lesion in the brain. Once we were operating on a portion of the brain called the cerebellum, which is located over the back of the head, just above the neck. The patient had to be seated with his head flexed forwards. Luck followed Murphy’s Law, which decrees, “What can go wrong will go wrong and at the worst possible moment”. In the midst of the surgery, the endotracheal tube or the tube which is inserted via the mouth into the trachea or windpipe, to ventilate the patient and deliver anaesthetic gases got dislodged and came out of the mouth. Because the patient was seated with a flexed neck and covered by surgical drapes, it was not immediately detected, until the brain started swelling and protruding out of the opening in the skull. Immediately the anaesthetist did the impossible of intubating or inserting a endotracheal tube in the seated position. Mind you that’s not an easy task and quoting Shakespeare, “All’s well that ends well”, the patient had an uneventful recovery.
The swelling of the brain was due to the buildup of carbon dioxide and lack of oxygen. Seeing an actual demonstration of this phenomenon made me realise the importance of oxygen in a head injury patient. The brain being already swollen due to trauma gets further swollen due to hypoxia or a lack of oxygen.
I learnt how to do craniotomies which unlike what is commonly believed about ‘brain surgery’ is fairly easy. First is to plan craniotomy according to the location of the lesion, then if possible to avoid crossing the midline as there’s the saggital sinus in the midline. The saggital sinus is a channel carrying venous blood enclosed by the dura mater. Also avoid going too posteriorly as the transverse sinus crosses there.
The logic being if you drill into the sinus you will encounter torrential bleeding which will be very difficult to control.
After planning the location of your craniotomy an incision has to be made on the scalp. This is in the form of a flap with a wide pedicle to prevent devascularisation or loss of blood supply to the scalp the flap preferably should be within the hairline as to be cosmetic.
A very popular question which is asked to residents in neurosurgery is ” What is the most important covering of the brain?” The answer is the scalp and not the skull as most people believe!
I encountered so many craniotomies done in other hospitals where there’s a defect in the skull covered by only scalp. Rather than cutting a flap of bone, a hole was nibbled in the skull and the scalp was sutured back over the defect. The patient is otherwise perfectly alright except for having a concavity on the head.
We treated this by sending the patient to the dental department where they take an impression of the defect and make a prosthesis, made out of the same material dentures are made of, to fit the defect.
The scalp again had to be opened and the prosthesis always fitted perfectly, sometimes it required some minor adjustments. The prosthesis was then anchored over the defect and the scalp closed. The patient had satisfactory contour of his head.
These days thanks to 3D printing a perfect prosthesis can be made to fit in the defect, like a hand in a glove.
Our plastic surgeon once used the flat bone from the ileum, which is the large bone deep to the buttocks. He only took just the outer layer of the bone along with it’s supplying blood vessel and placed it to cover a defect in the skull. The bone had a natural convexity matching that of the skull and the blood vessel was anastomosed or joined to the blood vessel in neighbourhood and voila! The patient had a living bone covering the defect.
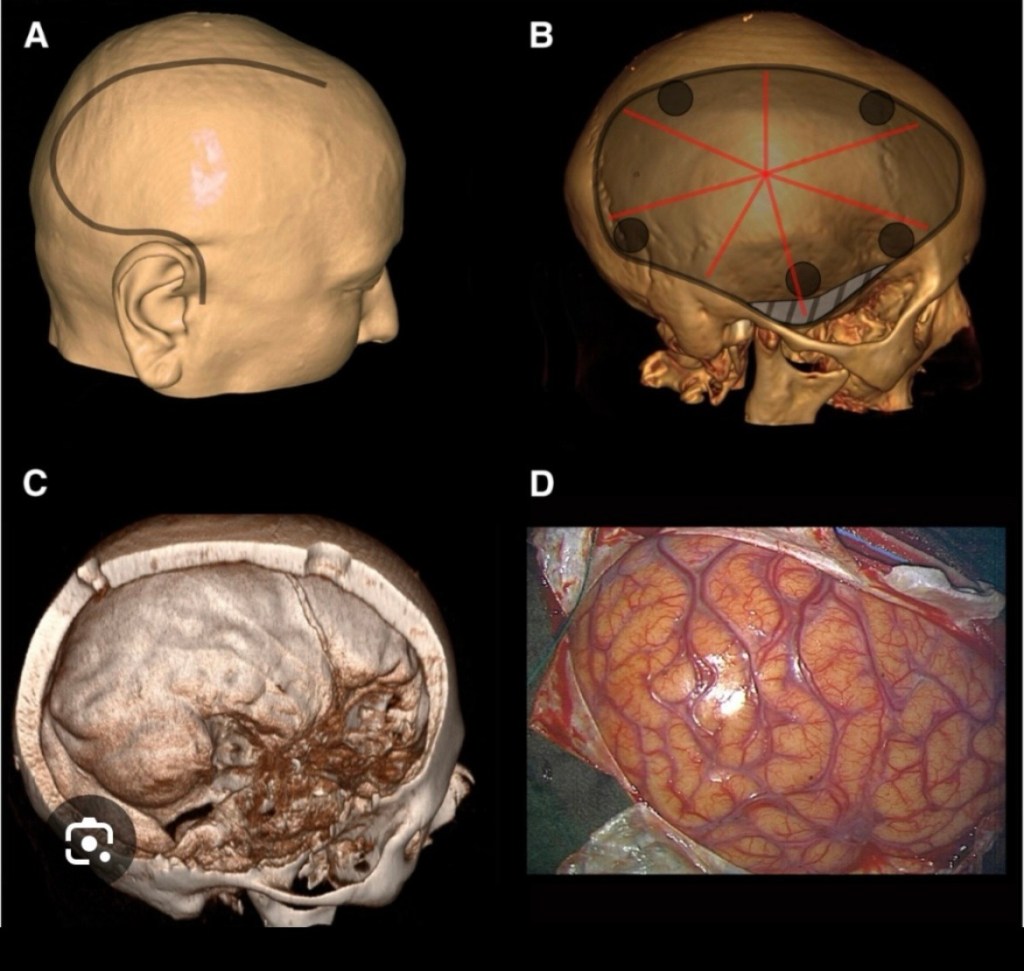
Returning to the subject of crainotomies, once the location is planned and an incision is made in the scalp, holes called ‘burr holes’ are drilled on the skull in a polygonal pattern, either pentagonal, hexagonal, octagonal or nonagonal pattern depending on the size of the opening required. While drilling the holes the dura mater is not punctured.
A. Scalp incision B. Burr holes C. Surface of dura exposed D. Surface of brain exposed
Then a Gigli saw wire is passed between adjacent holes and the intervening bone is cut. When all adjacent holes are connected a bony flap is raised having a polygonal shape. The advantage of having this bone flap was it could be replaced over the defect once the surgery was completed, avoiding the concave defect in the skull.
The Gigli saw is a very simple but versatile instrument. It consists of a thin, twisted stainless steel wire with serrated edges. Like a piano wire. It has detachable handles at each end for gripping. Designed to cut through bone with a back-and-forth sawing motion. It can easily threaded through two adjacent holes and the intervening bone cut.
Ironically it was originally designed by a Obstetrician and was used to divide the symphysis pubis in cases of obstructed labour, when Cesarean section was not safe.
Once the skull is opened, depending on the pathology, either on the dura mater or on or within the brain, an opening can be made in the dura mater to expose the surface of the brain.
I was gradually initiated, first I was allowed to make an incision on the scalp. The scalp being very vascular, the bleeding had to be controlled by holding the inner layer and everting the scalp.
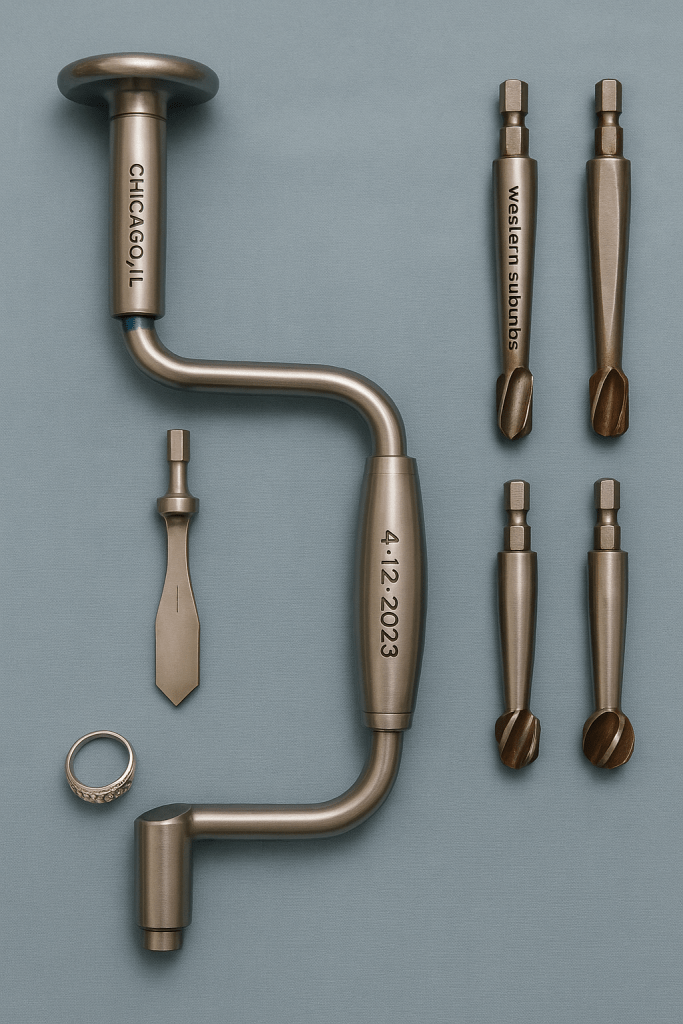
Next I was allowed to make the burr holes, this was done using what is called the’Hudson brace’ which essentially is like a carpenter’s drill. It had two tips, one is called the perforator which we use to penetrate the skull and the other is called the burr, which is used to widen the hole.
Initially the perforator is used till the thickness of the skull is penetrated and a small opening is seen at the base of hole. Next it is widened with the burr. It blunt tip but has bevels around it’s circumference and widens the hole.
Once burr holes made in a polygonal pattern over the skull we next got to join them with a Gigli saw. The wire of the Gigli saw is threaded through one burr hole and brought through an adjacent burr hole. Then the handles are attached and the wire is moved in a to and fro motion. The wire cuts the bone smoothly and once all the holes are connected, we have a bone flap which can be lifted off.
The skull because of it’s dome shaped design is very tough and does not fracture easily but the portion of the between the ear and forehead, behind the eye and above the zygoma or cheek bone is the weakest portion. This portion is called temporal region also colloquially known as the temple.
This area includes parts of several bones—primarily the temporal bone—and it’s a sensitive region because it has relatively thin bone and several important blood vessels and nerves running through it. That’s why a blow to the temple can be particularly dangerous.
In most martial arts the blows are aimed at this region as this can result in a KO or knockout. In Karate, Kung Fu and Muay Thai there is the round house kick which aims at hitting the temporal region with the side of foot or shin.
The protective gear worn is designed to protect the temporal region. Trauma to this region can result in fracture or in children who have an elastic bone just bending without breaking. On the surface of the underlying dura mater lyes the middle meningeal artery, the anterior branch of this artery is prone to injury and bleeding and an expanding haematoma collects in this region.
Before the advent of CT Scan diagnosis of an extradural haematoma was not very easy. A plain x-ray of the skull could show the calcified pineal body being pushed to one side. A cerebral angiography could be done which is injecting a dye which is radio-opaque into the internal carotid artery. An x-ray taken would outline the brain and demonstrate compression and deviation.
When there’s adequate suspicion an exploratory burr hole can be made on the side of the trauma. This is normally made just above the zygoma or cheek bone, midway between the eye and ear. You will encounter blood clots which will confirm your diagnosis. Then the same burr hole can be enlarged using a bone nibbler and the clot evacuated or burr holes made around it which are joined and a bone flap is raised. The advantage of creating a flap is there’s no defect and concavity in the skull.
With the advent of CT Scan things have become easy, a convex opacity is seen in the scan and the degree of compression and deviation of the brain from the midline can be assessed.
When my lecturer became confident in my abilities to do a craniotomy he allowed me to do a craniotomy for a case of extra dural haematoma. After reviewing the CT Scan he instructed me to make a ‘trauma flap’ on the scalp and then do the craniotomy. He drew the trauma flap for me, which started from the forehead on one side without crossing the midline and ran parallel to the midline posteriorly, then took a curve downwards and returns to end just above the ear.
I’m happy to say that the surgery was successful and the patient’s recovery was uneventful.
After completing my surgical residency I joined a hospital in a remote rural area, the population was 70% tribal. I had a lot of training but now was to put it into practice.
One night a young patient was brought unconscious to the casualty. He was a travelling salesman who sold blankets. He had gone to a nearby village to sell his blankets and had some altercation with the villagers who were drunk with the local brew ‘mahua’. One villager hit him on his right temple with a lathi. He lost consciousness momentarily but recovered and then went with his companions to register a complaint in the local police station. After registering a complaint he returned to the dharamshala where he was staying and lost consciousness.
His companions took him to the district hospital but they were unable to do anything for him. He was then brought to our hospital in the night, where the emergency doctors saw him and admitted him.
I saw him in the morning, he was deeply comatosed and both his pupils were dilated.
Going by the history of lucid interval I could come to a diagnosis of extra dural haematoma but since we were in a remote area we didn’t have the facilities for a CT Scan to confirm my diagnosis.
I was faced with a conundrum, if I referred this patient to the major cities which were 200 kms away, by the time he reached he would be unsalvageable. We had the equipment to perform a craniotomy so I explained the situation to the relatives and after taking they’re consent I proceeded on.
The anaesthetist said that he was so deeply comatosed that he would intubate him but not give any anaesthetic gases, only oxygen.
I positioned him to left side with right side of the head up. I first made a vertical incision over the temporal region and made a burr hole, I got got clots from the burr hole, confirming my diagnosis.
Next I thought whether to enlarge the burr hole or raise a bone flap. I opted for the bone flap. I made a trauma flap on the scalp and five burr holes around the first one. I joined the holes using a Gigli’s saw. Once I lifted the bone flap I could see the dark red clot. After evacuating the clot I could see the bleeding vessel which I ligated. Then I took stitches hitching the dura to the craniotomy opening. Then a drain was placed on the dura and the bone flap was replaced and the scalp closed.
By the time I finished the surgery the patient regained consciousness and began to move. The anaesthetist had to now supplement him with anaesthetic gases.
The patient made a dramatic recovery and only had hemipareisis or weakening of the left side of the body. This would also would improve with time.
I consider this one of the most satisfying moments of my career when I could use my knowledge and expertise to save a life. This was the reason why I became a surgeon.
The first time and place I met Sunil Agarwal was on July 17, 1978, outside the State Bank of India Extension Counter, Carmen Block. Our respective fathers had made the requisite payments for our admission. I clearly remember Sunil wearing a black and white checked shirt, grey pants, and polished leather shoes.
We said our goodbyes to our fathers and walked down the drive to the Mansion of Gods, carrying all our worldly possessions. Along the way, we were joined by B. Venkatesh, who was in the same group as Sunil. During that walk, we exchanged a lot of information. I learned that he was from Saharanpur, Uttar Pradesh—a place I had never heard of until that moment. He had completed his schooling at the famous Doon School and his junior college at DAV College, Chandigarh. Sunil Datta, who had also studied at DAV College, joined us.
We all decided to share a room in the Slums and occupied Room 119-120 for the duration of our first year. Sunil told us that his friends from Doon School called him “Agroo.” He was also known as “Junky” due to his bloodshot eyes.
During ragging, he was given a helmet with a Nazi swastika painted on it and a toy rifle. If anyone said, “Steady, Agarwal,” he had to retort, “Bugger all! Bugger all!” Because of this, he also earned the nickname “Buggeroo.”
Agroo was generous and never let his left hand know what his right hand gave. My first experience of his generosity was on the first night of ragging. We had to sleep on the floor of the upper common room, and the mosquitoes were eating me alive. Seeing my discomfort, Agroo handed me a tube of Odomos.
In those days, owning a music system was rare. Srideo Jha had a transistor. When he returned from our September break, Agroo brought a cassette recorder along with multiple tapes recorded at home. The company that made the tapes was Tony, a knock off of Sony. This provided much-needed music for Room 119-120, though the recorder rarely stayed in our room. Instead, it made its way around the hostel. Anyone who asked for it got it—Sunil never thought twice before lending it out.
He also paid mess fees for someone who couldn’t afford it and continued to help his dhobi’s family to the very end.
Saharanpur was known for its mangoes, and Agroo’s father, who owned a cold storage facility, would send a box of mangoes during the season. He shared them with everyone. At that time, we were living on the first floor of D Block, which had a balcony overlooking the hostel warden’s garden. The mango seeds landed in his garden, but unfortunately, they never took root.
While I was doing my bond Peter Desmond landed up in Nagpur and we went to Delhi to meet Bisoo in AIIMS. Peter had asked Agroo to lend his brother’s car to use in Delhi which Agroo consented. We travelled to Saharanpur and drove back to Delhi like Kings in a Maruti 800 but we ran out of petrol just before AIIMS and had to be towed by an autorickshaw to the petrol station.
We went like kings in the Maruti to the Grand Hyatt, though we could barely afford it but it. We met Afghan refugees from USA there but that’s another story.
Because of his public school education, Agroo could play all sports. He told us that it was compulsory in his school. He enthusiastically participated in cricket, hockey, and football. He wasn’t necessarily skilled at them, but he knew the basics and often clowned around, providing much-needed comic relief.
When it came to studying, however, he could read with full concentration, no matter the distractions around him.
Checks were his favorite. When I once asked him why, he simply said, “They go with everything.”
Initially, he always wore well-polished leather shoes. However, over time, the Vellore culture of wearing slippers and flip-flops won him over for its comfort.
My next close interaction with Agroo was when I was doing my MS in Ludhiana, and he joined the faculty as a Professor. He was liked by everyone—a rarity in Ludhiana, where very few people got along. Though there was no official system of foster children, he was immensely popular among students and “adopted” many. One of them, Edwin, followed his footsteps to Vellore and later became a vascular surgeon.
By then, Agroo had become a Vellore native. The language and mannerisms of Vellore had become part of him. He spoke Hindi with a South Indian accent, frequently using words like “chumma.” I remember him taking clinics for students and using “chumma” generously. The students suppressed smiles because, in the North, “chumma” means “kiss.” I remember his quotes “3 Ps of stopping bleeding are pack, pressure and pray!” I have followed it and re told it to my students. The last time I met him was in 2019, in Nagpur, when I was being installed as the President of the Nagpur Association of Surgeons. He gave a talk that was highly appreciated. Afterward, Agroo, Bisoo, and I visited Pench National Park. Though we didn’t see any tigers, we had a wonderful time.
Who knew that would be our last?
Delivered on 9th February 2025 at our online class prayers. I was corrected by Murli that the last time we met Agroo was November 2019 in Palghat Kerala.
One of my Professors made a statement which rings true to this day, “you can teach a ‘monkey’ how to operate and he will do a fairly good job, but what differentiates a monkey from a trained surgeon is, knowing the indications for operating and post operative care!”
Let me illustrate these points by a few examples, before I had joined MS course I worked as a junior doctor in a rural mission hospital. The hospital was well equipped and run by NGOs. One fine day the orthopaedic surgeon asked me out of the blue, “do you want to do an amputation?” Harbouring dreams of becoming a surgeon, I couldn’t wait to get my hands on a scalpel. I replied in the affirmative, to which he said “Gaekwad will teach you how to do an amputation”.
On the face of it Gaekwad did not seem to have the academic qualifications to be a teacher or for that matter, to operate. He had a high school degree and a certificate for rehabilitation of leprosy patients. But years of assisting various orthopaedic surgeons in the operating theatre had taught him the ropes. He was a patient and ‘respectful’ teacher, very unlike normal teachers who show scant respect to their students. It may have been my superior paper qualifications. So this student teacher relationship was on an unequal footing.
Thus began my first foray into a life with a knife. Though I was the one holding the scalpel, it was Gaekwad who was gently directing me, “Cut here, okay there’s a blood vessel here so tie it and a nerve here so cut it high”. Those were sound principles as if you leave the nerve long it could grow to form a neuroma and give rise to neuralgic pain over the stump.
In a limited field he was good. He may not be competent enough to do a complicated surgery but he was good at fractures and nailing bones, perhaps better than some orthopaedic surgeons. He did everything under the guidance and shadow of an orthopaedic surgeon. But the decision regarding the surgery or which patient would benefit with which surgery he would not be able to decide. In case there were complications following the surgery, he would not be able to handle it. What he was good at is to mechanically do the steps of an operation and with practice he had achieved a degree of perfection.
Fast forward 5 years and I returned to the same hospital with a MS general surgery degree against my name. I did all the general surgery operations leaving the orthopaedic work to the specialist. The orthopaedic surgeon was going on leave for 15 days and he asked me to look after orthopaedics during his absence. I confessed that I’m at sea regarding orthopaedics. His reply was “No problem you have Gaekwad and Titus to help you”. Gaekwad was considered the orthopaedic surgeon and Titus the orthopaedic physician. “If any patient comes with a fracture and only requires close reduction and plaster than the duo will do it. If it’s more complex requiring surgery then explain to the patient that we cannot operate immediately, because there is excessive swelling. He will require elevation of the limb and splinting followed by surgery. I should be back by then”. In this fashion I handled an orthopaedic unit, being the mere face of the unit whereas the grunt work was done by the duo. I looked after the general management of the patient. This is not unique as I have seen many orthopaedic surgeons dependent on technicians for placement of implants.
In this hospital there was a single qualified anaesthetist and two male nurse anaesthetists. These male nurses had done nurse anaesthetist course and were extremely efficient. They could give spinal anaesthesia, epidural anaesthesia, intubate the patient and even do single lung intubation. They managed the patients independently but were under the umbrella of the anaesthetist.
I like to give the analogy of an automobile engineer and your friendly neighbourhood car mechanic. The engineer knows all the theory, that the differential produces so much of torque etc. But he would be lost if you brought your car to him to fix. But the mechanic though may not know the physics behind the car engine design or would be unable to design a new car but by experience and trial and error, he fixes the car. He tightens some screws needs and some part needs to be gissoed (grinding) and will fix your car.
This is also true of a fresh MBBS graduate, who is bursting with knowledge but is at sea as far as the practical application of the knowledge goes. He learns the practical once he becomes an intern and is thrown into the management of patients.
When I joined as a surgical resident in Punjab, on my first call day I went to see a patient in the casualty. I met a ward boy (despite being middle aged, he was still known as a boy) in the casualty. He had been working in there since he was 18 years old and had risen from the rank of sweeper to ward boy. He greeted me warmly and told me that if I needed to do any emergency surgical procedures like tracheotomy (making an alternative breathing site in the neck), chest tube insertion (inserting a tube in chest for a collapsed lung) or venesection (inserting a intravenous line), he could assist/teach me.
He claimed to have a diploma in Ayurvedic medicine from Bihar by paying ₹400/-, which I suspect was fake. He always took the night shift which suited him but was unpopular with others, because he could practice ‘daktari’ during the day. I enquired what this ‘daktari’ entailed? To which he replied that he has his regular clients of rich business men or ‘lalas’, who were suffering from the problems of plenty like obesity, heart condition, hypertension and diabetes. He would administer their insulin shots and check their blood pressure. He also worked as a compounder for another doctor in the city, doing dressing, giving injections and dispensing drugs. He had his own clinic in the slum area where he lived and a devoted following of patients. He was Jodaram to us but his patients referred to him reverentially as ‘Dr. Jodaram’!
Once in a while a patient would stray into the casualty and ask for Dr. Jodaram. They would consult with him, show him a prescription given to them by some other doctor, for his opinion. He would then bring the prescription to me or to any other doctor present and say, “Doctor sahab yeh kya likha hai? Aaj meine chashme nahi laya hoon, padhna mushkil ja raha hai” (Doctor can you tell me what’s written, I have not brought my glasses hence having difficulty reading). Then I realized that he was barely literate, he could just about sign his name. He would ask what the drugs were for and whether they were appropriate and then convey the same to his patient. I wonder what he did for prescribing patients!
Another example in the same hospital was our head of plastic surgery’s assistant Rattan or ‘Rattanji’ as we had to reverentially refer to him. On my first days in plastic surgery posting, the Boss told me, “Rattanji and me are your teachers”. Rattanji was again a high school graduate but had the intelligence and aptitude to pick up things. The Boss used to perform specialized microvascular surgeries like reimplanting amputated limbs and fingers. There was one injury which was unique to Punjab. Since a majority had long hair, on Sundays they would wash their hair in the morning and leave it open to dry. Next they would start their agricultural water pumps to irrigate their fields. Very commonly their loose hair would get entangled in the spinning wheel of the pump pulling the hair and along with it avulsing the scalp from the cranium. Literally getting ‘scalped’. Patients would come to the Casualty with a bandaged head and holding a portion of the scalp with the hair still attached to it.
Another agricultural equipment which was a responsible for giving us patients was the ‘toka machine’. This was used for chopping stalks and chaff into small pieces to make fodder for the cattle. It consisted of a wheel whose spokes were sharp blades. The wheel had to be rotated and the bundle of stalk inserted slowly into wheel. The blades would chop the stalk into small pieces. Two scenarios resulting in accidental amputation of finger were, the person holding the stalk and pushing it into the wheel would accidentally push their finger along with the stalk into the wheel. After use if the wheel was not properly locked, to prevent the wheel from rotating, children playing with toka machine would get a finger amputated. The flip side of a toka machine amputation was that it was a clean slice and was amenable to reimplantation.
Toka Machine
Reimplanting scalps is difficult due to the multiple blood vessels, but our boss was very good at it. The only person he trusted to assist him was ‘Rattanji’. He knew the specialised instruments and how to assist. A wise person rightly said “To be a good surgeon you need to be a good assistant”. The assistant should know the steps of the surgery and anticipate what instruments or what retraction the surgeon would require. I sometimes equate it to a waltz where the dancing pair know the steps perfectly, when to sway pirouette and bow. But it should not become a Tango!
Rattanji was the perfect partner in the waltz, anticipating the surgeon’s needs perfectly. When the surgeon extended his hand he would know exactly which instrument he wanted without being told. When we had an exceptionally long list in plastic surgery we used to rope in Rattanji to do some of the minor procedures or suturing. He claimed he could do a cleft lip repair surgery and other plastic surgeries.
I am sure everyone in the medical field may have encountered a version of ‘Dr. Jodarams’ and can recount the case of a paramedical staff who was as good as a doctor in a limited field.
If I can summarise the life of my mother, it would be, ‘A long and fruitful life, where she touched many lives positively and made a differences for the better’. Iris Wilkinson was born and raised in Allahabad, UP, where she did her schooling. For higher education she studied in Isabella Thoburn college Lucknow where she met my father and got married. They moved to Nagpur in 1958. She taughted in St. Joseph’s Convent until she retired in 1990. Scores of her students remember her fondly for being gentle and soft spoken but also firm. She was very approachable. Many students approached her for advice. Her suggestions were always very practical. One of her students whose name is Jumana, herself recounted this story. She complained to my mother that another girl constantly teased her by calling her Jurmana. My mother asked her what was the girl’s name? ‘Chadha’ she replied . My mother suggested “just call her chaddi and she will stop teasing you”. And it worked like magic! Along with her regular job she was also managing the orphanage of the Diocese, the Shishu Sangopan Griha. She told me that working with the orphans and abandoned children was the most fulfilling thing in her life. There was a time when she kept the new born babies who were most vulnerable in our house. So there was a row of cribs and a caretaker who worked under the watchful eyes of my mother. Many of these children were adopted by families in the Netherlands and Norway. Annelies who is present here adopted two beautiful girls from Shishu Sangopan Gruha, who are now mothers themselves. All of these children when they met my mother, despite the passage of time, felt and instant connect and chemistry. They now consider her as their Indian mother. My mother and Annelies founded Navjeevan Sanstha and the Dr. T.S. Wilkinson Memorial school. The logo is hands holding a diya and the motto is to lead to the light. My mother used to see children begging outside the church after services. She discovered that in Government Schools nothing was taught so they lacked even the basic knowledge and no motivation to attend. She felt they require one wholesome meal a day as an incentive. So the school started initially on rented premises. In the Chatterton Hall at first. There were days when the hall was booked by other people, then my mother conducted classes under the trees in this church compound. Because they were dealing with street children no one was willing to rent out premises. With the help from donors in Netherlands they were able to make a residential school in Godhani, which now has 200 students. Many of the ex students are now employed as nurses, accountants and technicians. These are the success stories. My mother was happiest when she was visiting the school and like a child refuse to return home. It’s only in the last few months her health deteriorated and she was confined to bed. Ultimately nobody runs forever and her time had come. She is definitely in a better place now. In conclusion to quote 2 Timothy 4:6, which would be apt for her life. “I have fought the good fight, I have finished the race, I have kept the faith.”
Dear Fiends! We are the lucky ones to still be around for the 45th reunion of our Batch. Time has literally flown. On 17th July 1978 when we entered the portals of CMC, the five and a half years for our course, seemed like infinity to me. A senior doctor saar of the ’73 batch put it in perspective, “Dei! When I joined in first year you were in 7th standard!”
Those who have read my blog, and for those who haven’t, on the perception of time. I had postulated that perception of the length of time is inversely proportional to your age! At 1 year a year represented your entire life, at 5 years it was 1/5th of your life. As you age that fraction shrinks as the denominator increases, now it’s 1/62 for most of us. Our perception of a year has proportionately shortened. I have driven down to Bangalore from Calcutta with the King of Calcutta Bong Biswas and his beautiful wife Neena. We broke journey in Horsley Hills trying to recreate the nostalgia of our class retreats. The place is unrecognizable with tourist and trash but still retains some of the old world charm of a British hillstation. We could not locate our retreat centre apparently it does not exist anymore. We searched for the iconic rocks on which most of our old pictures are taken but it was futile.
Bangalore also brings back nostalgic memories of 1976, when our family had driven down in our family Ambassador. That was my first trip south and exposure to the language and culture. Road trips then were a different story then. The cars were not air conditioned and there were limited amenities on the highway. When we reached Bangalore we were surprised with the cool climate. There were no fans in the place where we stayed, it was considered too fancy!
We were quite amused that a ubiquitous road like Mahatma Gandhi road found in every town in India, was given a modern spin and called MG road! It removed the image of and a bent doddering old man with his cane and instead conjured an image of a modern happening place. Appropriate since MG road was the happening place in Bangalore.
At that time all along MG road there were posters advertising the latest hit Kannada movie, starring the superstar of Kannada movies, Dr. Raj Kumar. The story was based on Shakespeare’s ‘Taming of the Shrew’ and had an apt titled, ‘Bahadur Gandu’.
In Hindi, gandu would loosely translate to an asshole and bahadur means brave. It is logical that a man has to be brave and an Asshole to attempt to tame a shrew, invariably his wife.
While on the subject, I remember the old joke about how all the parts of the body fought for the position of the Boss. The brain the ears, eyes, mouth and nose staked their claim. The anal sphincter aka the asshole also threw his hat in the ring. The others laughed at the anal sphincter who sulked and refused to function. The brain became feverish, the ears began ringing, the eyes saw blurred and the mouth could not eat. They all appealed to the brain, “Let the asshole be the Boss!”. And it came to pass that the asshole became the Boss. All the parts of the body functioned perfectly and the asshole did nothing at all, except pass out a lot of shit. The moral of the story is “You don’t have to be a brain to be the Boss, being an asshole is sufficient”. I recollect a quote by Dean Martin “At my age the biggest satisfaction is having a decent crap in the morning”. I am sure many of us would concur.
In our vast country with various languages one word may be inoccous in one language maybe noxious in another. For example imagine my hard core Malayali mother in law’s indignation when she knock on a door and the occupants told her, “Kundi khole ke andar aa jao”.
After I completed my MS, I forayed into private practice by necessity. My mission hospital paid peanuts and I had a family to support. Being a bottom feeder at that time, I was left with, what else? The bottom! All the anal fissures, haemorrhoids, fistulas and perianal abscesses not to forget the fecal impactions came to me. This region people higher up in food chain would not touch with a barge pole because they had the thyroids, abdomens, appendices, hernias, hydroceles and of course the breasts.
Like the motto of a gynaecologist is “Always at your cervix!” mine was “Always at your a____e”, you guessed it right. I went about my job in earnest and became good at it, remembering the famous quote by Bailey and Love, “If you don’t put your finger in, you will put your foot in.” This must have been told to us ad nauseum during our MBBS. There were anecdotal stories of the great Puli and his penchant for p.r.s. A Princess from the Royal family of Nepal admitted in M ward with pyrexia of unknown origin. After taking an extensive history and doing a thorough examination, Puli did his famous p.r. and Eureka! He found a perianal abcess, which was the cause of the fever. When we were in CMC I remember most of the patients with perianal problems were from across the border Andhra Pradesh. It was attributed to the fiery Andhra food. In Nagpur we have our own very fiery ‘Saoji cusine’, which is supposed to beat Andhra cooking hands down in terms of conflagration. People have devised an informal grading system for the degree of heat. Grade 1. Mouth on fire. Grade 2. Stomach on fire. Grade 3. Morning after rear end is on fire. A young adventurous Vellaikara white man visited Nagpur and being either bahadur or foolhardy, he decided to experiment with Saoji cusine. The moment he took a bite his face turned crimson and he opened his mouth and stuck his tongue out and fanned it with his hand. He gulped down at least a gallon of water and gripped his abdomen complaining of burning. Morning after when he sat on the water closet he passed few hard lumps followed by intense burning. By his description the pain was like passing out a barbed wire! He reached for the toilet paper to wipe himself but the rough paper behaved like an abrasive, making matters worse. He then spotted the hygienic shower and aimed it at the afflicted area. That was an epiphany moment, he realized why Indians wash it rather than wipe it! He visited me the next day still complaining of a persistent burning. I asked him to strip and lie down in the left lateral position with his right leg flexed. First thing I noticed was a realistic lipstick mark tattooed on his right gluteal region, which seemed to imply either “kiss my ass!” or “my ass has already been kissed”.
On digital examination I felt button hole like abrasion in perianal region, diagnostic of a fissure in ano. He was send off with a prescription of smooth muscle dilators, laxatives and soothing sitz baths.
On the subject of wiping there is the story of a senior anaesthetist in CMC being reprimanded by a white theatre nurse for resting his backside against the shelf containing the autoclaved drums. “Kindly remove your unsterile backside from my sterile equipment” was her reprimand. The anaesthetist not short on wit retorted, “Sister we wash it and don’t wipe it”.
This satirical essay was written by a former resident describing his journey through surgical residency. He describes his trials and travails with sardonic humour. He prefers to remain anonymous.
Sinbad had done his MBBS from a Medical College in Dakshina Kannada. An average student but often marked out by Professors as someone with ‘great potential.’ It was in internship that he had found his inner calling- Surgery. He loved the smell of spirit and the sight of blood and pus. He was quite eager to dress the burns patients and if ever a resident offered him a lacerated scalp to suture, he would gush about it for the next many weeks. The one time he was told his suturing was better than the residents’, he relived the procedure throughout the night. He enjoyed the company of surgery residents- there was something about them which was different, cool, macho.
The Professors had their quirks but were legendary- to see Dr. Thangam Varghese operating was to see an artist paint, Dr. Sri Ram Bhat’s left hand was spoken of among interns as much as his book was appreciated, Dr.Harish Rao’s diction, Dr. Ashfaque Mohammad’s humor, Dr. BM Nayak’s jogs and intra-op high-fives, Dr.SP Rai’s conduct. He certainly wanted to be a surgeon.
It isn’t clear where he spent the next two years. But he was preparing for the post graduate entrances. His seniors had advised him not to take up any clinical jobs, for they had understood that it was difficult to work and study for NEET simultaneously. As he wrote his first set of examinations he realised a cruel fact. They do not ask you what you should know in entrance exams. It is merely an exam of elimination to aid the filling up of post graduate seats. And so he wrote-ten, twenty, thirty, forty exams and more, across India, in two years and failed in almost all of them, qualified a few but was knocked out at the interview stage in a couple of others. Two years of loneliness, failure, rejection, helplessness and the lack of an identity.
This was when the heavens woke up to his pleas and he found himself a seat in Surgery, somewhere in North India. The years of misery were over. The Promised Land, the land of milk and honey awaited him. And unlike many others, who wanted Orthopaedics or Medicine or Radiology but were settling for Surgery owing to their ranks, he had actually found himself in the field he loved the most. This was going to be tiring but rewarding, or so he thought.
This was what he learnt in Residency.
First Year:
Humiliation is a way of life here. Most things you are shouted at for aren’t even your fault. Shouting at you portrays the Boss as a sinless God in front of the patient. Your senior can scream at you in public for his own fault and you shall put your head down and listen.
It’s all Divide and Rule brother. All the powers that be need do is make your passing conditional to their approval.That is enough for colleagues to find every opportunity to put another down through three years.
Do not trust your own brother if he is your colleague or senior. Nobody is here to learn Surgery the way you thought they would be. In an environment of insecurity, do not expect anybody to keep your secrets.
They will be polite to their wives and children for they need to be. They will be polite to their patients, for they are their livelihood. They will never be polite to you. You are the scum of the earth.
They will say do not eat till the job is done, but make sure you eat. Especially breakfast. They will not care whether you slept in days or not, but will disturb your sleep at midnight by taking an additional round, merely to feel senior.
Hydrocele is your cutting. Unless the Boss decides he wants to teach a beautiful intern what a tunica vaginalis looks like. And this will happen often. If your eyes brighten up at the sight of a hydrocele, teach them not to. Don’t blame the intern, put her to good use. If she can chat up the Boss in OPD, that will save you from a lot of pedal lactic acidosis.
Touch feet as often as possible. Even if your back hurts. You touch feet for years and then you get your feet touched for years. It means nothing. Just keep touching. Makes life easier.
If a wound gapes, it’s your fault. Seroma, Haematoma, Surgical site infection. All of it your fault. Even if you were not present inside the operation theatre and did all you could to prevent it.
Take time out to cry. You need to keep your system light. You might struggle from suicidal ideation, but it is documented that 30% surgery residents do too. So you are not alone. You can always jump off the hostel building like many before you have, but that won’t change the way things work around here.
Don’t work hard. Give an impression that you are hard-working. Both are two different things. Work where you can be noticed, when there is maximum possibility of being noticed. Exert yourself completely to the patient who is Boss’ relative/ mechanic/ driver. Your elaborate burn dressings will never be seen, don’t even bother.
Curiosity and Spirit of Enquiry is all bovine faeces(bull). Never ask questions. Be a YES man. It’s good for your health.
Second Year:
Get a car. Boss has his income. But Boss likes to save. Drive him around. Feed him till he chokes. Your father’s hard earned currency notes are actually confetti meant to be showered on Boss.
If he asks you to buy him a brownie, get him ice cream too. If he asks you to buy him a helicopter, buy him a space station. Why? He knows many ways by which he can ruin your life. He is Boss. The medical establishments have no way of assessing and admonishing the dinosaurs in the food chain.
Your senior is exam-going. He needs a good impression. Take the blame for his mistakes in the morning. You can always whip the juniors in the evening. Or tear up their files.
Hernia is your cutting. Unless the Boss decides he needs to teach an undergraduate damsel how a tension-free mesh repair is done. Or, the Lecturer would be in a mood to finish three hernioplasties under 45 minutes by himself, some silly personal record of his . You will be second assistant forever, or so it will feel. Don’t run throughout the night trying to get the patients fit for surgery. You will get peanuts at the end of it.
Lecturers don’t care about you more than they care about their job. And for many reasons they need to be in Boss’ good books. Else he’ll load them with more cumbersome work and stall their promotions. So anything you tell them in good faith shall be duly reported. And if they tell you something personal, they are merely venting. Don’t read too much into it.
Humour in Surgery sucks. It is almost always slapstick. Almost always centred around boobs and balls. Few get sarcasm and almost no one will understand a pun. The older they get, the more funny they try to be, the worse the humour that comes out. Laugh anyway. Else you stand out as a sore thumb.
Start holding the Boss’ suitcase as he walks in and walks out. Go up to the car. It is all a colonial hangover. It makes absolutely no sense, but do it anyway.
Anaesthetists are almost always women. They almost always are in a rush the moment the scalpel or needle-holder is thrust in your hands. She will insinuate your lecturer or boss about how fast things would have gone had he been operating. Your superior is hormonal. He takes her comment as instruction. Walk over to the other side buddy, again.
They’ll say how their residency was far busier, far superior and far fetched things like how they did Whipple’s alone in a dark room under local anaesthesia. You’ll wonder why they don’t teach you how to drape, hold a needle-holder, place a suture. Never vocalise it.
Flatter. Suck up. You’ve never done it? Well, now’s your time. Flattery always works. Remember, your goal is peace of mind. Nothing else.
Third Year:
Do not ask for surgeries. Ever. Somebody in the food-chain above you will wait till you make the smallest of blunders, and then announce it to the whole wide world. This, despite you going out of the way to hide their own errors from them, and others, for 2 years now.
If you are complimented for your work, deflect it to someone senior to you present nearby. Some patients will want to tell the world how much you have helped them, make sure they do not reach Boss’ ears. He sees you as competition, not as a disciple.
Almost all surgeries in the operative list are supposed to be your cutting. Don’t believe it? Check your logbook. But of course, now that you do not know how to do a hernia well, how can they trust you with a mastectomy or a thyroidectomy. You should have worked harder in your residency. For now, you get nothing.
Buy costly stuff for Boss and his wife. Give it to him as a Diwali present. He will refuse. But that is a token refusal. He is an abyss. Coax him till he takes it home. You need your thesis signed.
Stop entering the O.T. Boss doesn’t think you need to learn surgery nor does he think you need time to study. He will remember to make you write his wife’s research article days before your university exam. Stay out of his sight, stay out of his mind.
It’s a tree of monkeys. Your senior will see only monkeys below him. Your junior will see only Hilton-lined holes above him. The cycle continues.
They’ll tell you observation is learning. It is, but it is not. You can observe a hundred perforation closures but still think of it as an insurmountable mountain. It is only when the scalpel and bovie are in your hand do you learn the trade, which you probably won’t till you are here.
Sinbad received a call from his Boss weeks before his University exam that he was going to be failed. Thanks to the insistence of two Senior Examiners who voted against the pre-meditated verdict, he was passed, in his first attempt. The God who saved Peter from drowning had saved him too. He has come to appreciate the few friends that stood by him in residency, the love of his life was a God-sent balm, his parents helped him stay sane with their regular visits and daily prayers. Now he works in the suburbs under a kind mentor- learning to drape, suture, operate. He insists that not all residents are selfish, lazy and lacking in passion. Some lose their passion in residency.
Tuesday, 8th February 2022 at 5:30 pm NS, a 25 year old photographer by profession, stepped out of his house in Bhim Chowk, Jaripatka, Nagpur. Little did he know what fate had in store for him. Aptly demonstrating the unpredictability of life.
He was rushing for an assignment at a tony Hotel in the city. He was dressed to the nines with freshly coiffure hair, spiffy clothes and a gold chain around his neck. He got on his two wheeler and because he was running behind time, he drove at a fast pace. The route took him through crowded localities with narrow lanes.
A month had passed from Makar Sankranti when traditionally kites are flown but there were some stray kites still flying from the roofs of houses. Suddenly NS felt a sharp piercing pain in his neck. He had been snared by a stray kite string, suspended across the road between two buildings. The string dragged him off the vehicle and onto the ground. The vehicle drove driverless for some distance before toppling over. He put his hand on his neck only to find his hand covered with blood. He could feel a huge gash across his neck which was bleeding profusely. He immediately took out his handkerchief and tied it around his neck. Meanwhile bystanders gathered around and began clicking pictures and videos of the accident. He tried to appeal to them for help but no sound came out of his mouth, only wind escaping from his neck with gurgling sound. The thread had cut through his neck and severed the trachea or wind pipe below the vocal chords rendering him literally voiceless. He was a victim of the killer string, the infamous Chinese Manja.
Cut with the open trachea
Makar Sankranti, Uttarayan, Maghi or Pongal as it’s called in various parts of India, marks the entry of the sun into the ‘Makar Rashi’ or Capricorn. This normally occurs on 14th of January on non leap years and the 15th on leap years. It’s celebrated in various ways, from bonfires, sweets to flying kites.
The cotton string of these kites were traditionally treated with a mixture of rice paste and tree gum as binders, mixed with powdered glass got from crushing tubelights or bulbs, dye and other secret exotic ingredients like the contents of a torch battery. To coat the string with the mixture it is strung between two convenient poles, a lump of the mixture was rubbed along the length of the thread allowing the thread to get coated. To avoid the applicator’s fingers getting cut he wears small tubes on each finger or taped his fingers. This sharp string is called ‘manja’.
All these preparations were for the traditional kite fights. The kites are maneuvered so that the threads of two kites would get entangled in an embrace and rub against each other or ‘pech ladaana’ as it’s known in local parlance. One of the kite’s string would get abraded due to the friction and the kite would float loose. In Nagpur this is followed by a shout in unison by the people flying the victorious kite, “O paar” or “O kaat” depending on which part of the city they’re from, which means the kite is cut. In Gujarat the shout is “kai po che”.
Then there are the kite runners, consisting of children and even adults, scanning the skies and waiting for a kite to go adrift. They chase the kite armed with long bamboo poles having a dry thorn bush tied to the end, to snag the kite thread and claim the kite as a prize. This is called ‘patang lootna’ or looting a kite. The kite itself has hardly any value but the looting was part of the fun and tradition. Then there are the Sharayati, people who place bets or sharayat on which kite will be victorious. Huge sums of money exchange hands.
Behind this seemingly innocuous sport there is a sinister undertone. In a quest to have stronger and sharper manjas, in last 10 years the traditional cotton string was substituted with nylon string, the so called ‘Chinese manja’. Despite it’s name the Chinese manja is not necessarily from China. It is a desi spun product but given that moniker because it was cheap. The fibres, maybe imported from China. This manja is coated with glass and metal filing and is extremely sharp and unbreakable. This manja is capable of slicing through flesh like a hot knife through butter. Unlike the cotton string it is not bio-degradable.
The kite strings get strewn around trees, between buildings, lamp and electric poles. If it crosses a road and an unsuspecting person on a two wheeler gets snared by it, it’s capable of inflicting deep wounds. Invariably it slides over the body but gets hooked at the neck and cuts through the neck. The traditional cotton manjas were sharp but had a low snapping point. They caused damage but not usually deep. The Chinese manja has a very high snapping point enabling it to cut deep and inflict damages.
The kite runners while chasing kites grab on to kite strings which may cross the road and injury an unsuspecting two wheeler rider. The kite runners are so intent on looting a kite that their are oblivious of the traffic and can get hit by a passing vehicle. They also position themselves on rooftops to have an advantage of height to grab onto the string. Fall from buildings are very common. I have treated a small boy who fell from the roof of a house and his thigh got impaled on the spikes of a gate.
Then there’s the betting by the Sharayatis. Betting is illegal but the authorities turn a blind or Nelsonian eye to it. Because winning involves not getting your kite string cut, the demand for the stronger Chinese manja shot up. Now no one can survive a kite fight without using the Chinese manja because cotton manja stands no chance against it.
The manja being non degradable poses an environmental hazard and to birds who also get entangled in it. The National Green Tribunal declared a ban on this manja. But despite the ban, it’s observed more in it’s breach. The Chinese manja can be easily brought in the black market or it is sold in the guise of industrial use.
There were a sequence of events which saved NS’s life. You can call it fate or an act of God or as the Hindi saying goes ‘jako rakhe saiya, mar sake na koi’ (A person blessed by God, cannot be harmed) .
The first was a friend of NS happened to be passing by the accident site and when he saw NS he immediately rushed to his aid. He hailed a passing e-rickshaw and took him to the nearest hospital, which was Janta Maternity Home and Hospital.
The second event was I normally have my consultation in Janta Hospital at 7 pm but that day I had to attend a meeting at 8 pm. I decided to go to Janta early and see my in-patients and miss my evening consultation. I parked my car near the hospital and walked to the gate. I saw an e-rickshaw coming at speed to the gate and attendants lifting a young man off the rickshaw and on to a waiting gurney. The clothes of the attendant were blood stained and the patient’s clothes were soaked with blood. I was told he is a victim of the infamous Chinese Manja. I immediately went along with the patient to the casualty and shifted him onto the examination table. On removing the handkerchief covering his neck, I was greeted by a gush of blood and a spray of blood mixed secretions from the transected trachea or wind pipe, as the patient coughed.
I thought for a moment, “this is way beyond my league!” and the thought of referring the patient to a higher centre briefly flitted through my mind. But then I saw a young man just beginning life, pale as paper, pulseless and a barely recordable blood pressure due to exsanguination . If I referred him in this condition then death was a foregone conclusion.
I recalled an incident during my surgical residency days, an ECG technician stabbed a Microbiology technician in the hospital campus due to personal disputes. The ECG technician knew the anatomy of the heart and stabbed him just below the left nipple, directly in the left ventricle of the heart. What saved him was he was immediately taken to the casualty and a cardio thoracic surgeon was available. The cardio thoracic surgeon took the bold decision of immediately opening his chest, between the ribs, at the site of the knife wound and controlling the bleeding with a stitch on the left ventricle. Once the bleeding was controlled he could be transferred to the operation theatre for a formal surgery. All done sans anaesthesia but the patient was knocking on heaven’s door and was oblivious of pain. This bold action saved a young life!
In Advanced trauma life support (ATLS) training in trauma medicine, there is the ‘Golden Hour’ concept, it is the period of time immediately after a traumatic injury during which there is the highest likelihood that prompt medical and surgical treatment will prevent death and reduce morbidity. I definitely didn’t have an hour to act so no time should be wasted. I went through the ABC of ATLS, which is airway, breathing and circulation. I asked the junior doctors and nurses to start an intravenous line and rush in fluids, administer oxygen and send a sample for immediate cross matching for blood.
I explored the wound to find the source of bleeding, the external jugular vein which was severed on the left side and was pouring blood. I managed to clamp and tie it. There were other smaller bleeders which could be tied off, luckily other major vessels like the carotids or internal jugulars were intact. Now I had a relatively bloodless field and could assess the damage. The trachea had been almost completely transected and was acting like a tracheostomy through which the patient was breathing. I covered the wound lightly with sterile pads and shifted him to the operation theatre. An urgent call for the anaesthetist was sent. I went out and spoke to the relatives, I told them he has a fifty-fifty chance of survival and I will give it my best shot and the rest is in the hands of the Almighty.
In the operation theatre I injected local anaesthesia into the wound and began suturing without waiting for the anaesthetist. The trachea does not have any sensation, I first sucked out the clots and blood in the trachea with a suction, the patient coughed reflexively. Then I began suturing the trachea, with 3 stitches the transected ends came together. There was no air leak and the patient began speaking. Now he was able to inhale the oxygen which was being delivered to him via a face mask. The first thing he said was that no one came to his aid at the accident site. Next I began suturing close the strap muscles of the neck and followed by the platysma which is a muscle just below the skin and finally the skin. His vital parameters like blood pressure and oxygen saturation improved. We finally felt that he was out of the woods.
Immediately after suturingThe next day Two subsequent days
The patient made a miraculous recovery, he was up about and talking by the next day. He kept in intensive care unit (ICU) and monitored for possible complications like aspiration pneumonia from blood entering the trachea. But luckily his recovery was very smooth.
To quote Shakespeare “All’s Well That Ends Well”. I was lauded for my timely efforts which saved a life. But suppose things went bad? The same people would have criticized me for ‘biting more than I could chew’. The same relatives who touched my feet declaring me a God could have become violent. A patient living or dying is not in our hands, we can do our best but ‘there’s many a slip twixt the cup and the lip’. But ‘fortune favours the bold’ and I got a once in a lifetime chance to save a person’s life. As a doctor and a surgeon that’s what I was trained for. We should never shy away from being the good Samaritan.
News report
One of my classmates sent me this message, “Wow, impressive! Tell us more:
How did you manage the airway to prevent aspiration without an ET tube? I see only an O2 mask
Why under local? Was there no anaesthesia help available?
If you had intubated through the mouth and got the end of the ET tube into the distal trachea and inflated the cuff, could it have prevented aspiration and served as a tracheal stent as well?
Could he have been transferred to a higher centre where specialist anaesthesia help was available? Why the decision to repair immediately under LA?”
My reply was : “I work in a depressed area which has mainly a slum population. Luckily I was in the hospital when the patient was brought to the casualty. His external jugular were severed on the left side and he was in shock. Initially I planned only to resuscitate him. I caught the bleeders and started iv fluids. The trachea was lying open and already blood had gone in which I aspirated. The anaesthetist meanwhile had not yet arrived so I thought I’d close the trachea to avoid further aspiration. Once I had done that then I sutured the strap muscles and closed the wound. He was not in a condition to be immediately transferred and he would not have been able to afford a corporate hospital. The government medical colleges are in shambles, so I took the decision of managing him myself after taking the relatives in confidence.”
As we stepped into Men’s Hostel on 17th July 1978, we were told to meet the Hostel Secretary for room allotment. The Hostel Secretary had commandeered a vacant room and was seated behind a desk. He handed us a form which we had to tick our preference for room, ‘double/single/single with attached toilet/single with attached toilet and AC’. I wisely decided on single though in the hot and humid Vellore climate, AC was tempting but I somehow knew it’s highly unlikely that there were AC rooms.
Later I was grateful for my decision because during initiation those unlucky ones who opted for a single room with attached toilet and AC, had a pipe strapped on his back with a shower head suspended above his head and a bed pan tied around his waist as an attached toilet. An aerosol can was suspended around his neck as an AC.
The dream of an attached toilet was always in the minds of the residents of Men’s Hostel, the luxury of not having to walk down the corridor to the common toilets. It was like having the keys to the executive washroom.
During bacchanal parties, indulgence caused increased diuresis and delay. The urgency was so great that they barely managed to step out onto the corridor, and relieve themselves over the railing, which was at a convenient height. The car of the hostel warden parked in the driveway in ‘D’ Block was a regular beneficiary of these ‘showers of blessings’.
This idea may have been instilled in our minds during initiation, when following our morning exercise supervised by the ‘Field Marshal’ and ‘Executioner’ we were supposed to in batches of 3, lie face down in front of ‘C’ Block store and chant in unison, ‘God! God! Give us rain!’ Our prayers were answered when a bucket of water was poured on us. Then we rolled in the mud and again appealed for rain. During this ritual I felt a thin stream of water hit me which had a warmer temperature, suspiciously close to body temperature. Some seniors shouted, “Don’t piss on the poor buggers!” I went berserk and tried to look up but my head was promptly pushed back into the mud.
A story which made rounds in Men’s Hostel and was part of folklore that there an occupant of supertop who routinely used to relieve himself over the railing, fouling things up for the occupants downstream. No amount of entreaty would make him mend his ways. So the occupants downstream took matters in their own hands. They got an electric stove, the ones which had the glowing coils, placed it on an old badminton racket and tied a bamboo to the racket. The stove was plugged into an extension cord. Then they waited patiently for the nightly flow of effluent. When they heard the pitter patter of effluent hitting the ground they switched on the stove and extended so it was right under the stream. It was the perfect ‘mid-stream clean catch’, the stove sparked, the stream stopped and cry of pain was heard from above. To make a long story short they were never troubled again by the flow of effluent.
Then they were the improvised chamber pots, after all “need is the mother of invention” and the desi jugaad in keeping with “waste not want not”. There were a vast collection of empty bottles from past revelry in the hostel rooms, which were put to good use. They were refilled capped and placed in a hidden corner under the bed. Once in a while the watchman would come to sweep the room. The watchman in his attempt to reach the dust in all corners reached the cache of refilled bottles. He picked one up, shook it, looked at the it and stopped just short of sniffing it. Then gave the owner an incredulous look and asked, “Idhu enna Saar? Urineaa?”
Do the past residents of Men’s Hostel, especially Circa 1978-1984 recall the strange malady which befell only the males called ‘calcium trouble’?
The clinical scenario was after vigorous and sweaty physical activity or on a hot sweaty night, the victim goes to the toilet to pass urine but is alarmed that he’s unable to pass urine. Just a few drops emerge with severe burning in the urethra.
The treatment of ‘calcium trouble’ paradoxically was common salt. The victim would rush to the mess, pick up the salt container placed on the dinning table, go to the water cooler, pour a glass of cold water, add a fistful rather than a pinch of salt. After one or two glasses of this mixture he would return to the bogs. A blissful expression could then be seen on the suffer’s face along with the sound of urine flowing freely.
It was said that due to the high calcium content of the drinking water which caused this form of dysuria, hence the dubbed as ‘calcium trouble’. How common salt relieved the suffering was a mystery.
During initiation after our exercise session we were told to drink water with salt. I always thought this was part of the initiation but later discovered the reason.
After any physical activity in the hostel, the ritual was the players would run to the water cooler with salt and drink one or two glasses.
Luckily I only had an attack once during my tenure in CMC. But there were others who told pitiful tales of painful peeing and implored us to take precautions. Hence it was water with salt on a regular basis. I suspect I can blame my early hypertension to this practice.
Now the water drunk I am sure undergoes, reverse osmosis, filtration, ozone treatment and God alone knows what else. Plus bottled water is the norm, so I suspect this malady has become a distant memory or an idiosyncrasy of the Batches of yore. In those simpler times water was straight from the tap.